Kidney Function & Drug Dosing Calculator
Calculate Your Kidney Function
Results
Dosing Adjustment Guidance
When kidney function is reduced, your healthcare provider may need to adjust your medication dose. The exact adjustment depends on the specific drug and your overall health.
For many common medications, a 30-50% reduction in dose is needed when kidney function drops below 50 mL/min. This helps prevent side effects while maintaining therapeutic benefits.
Ever wonder why two people taking the same pill at the same dose have completely different experiences? One feels fine, the other ends up in the ER? It’s not luck. It’s not magic. It’s pharmacokinetics - the science of what your body does to a drug. This isn’t just for doctors and pharmacists. If you’re on medication, even once, this affects you.
What Happens When You Swallow a Pill?
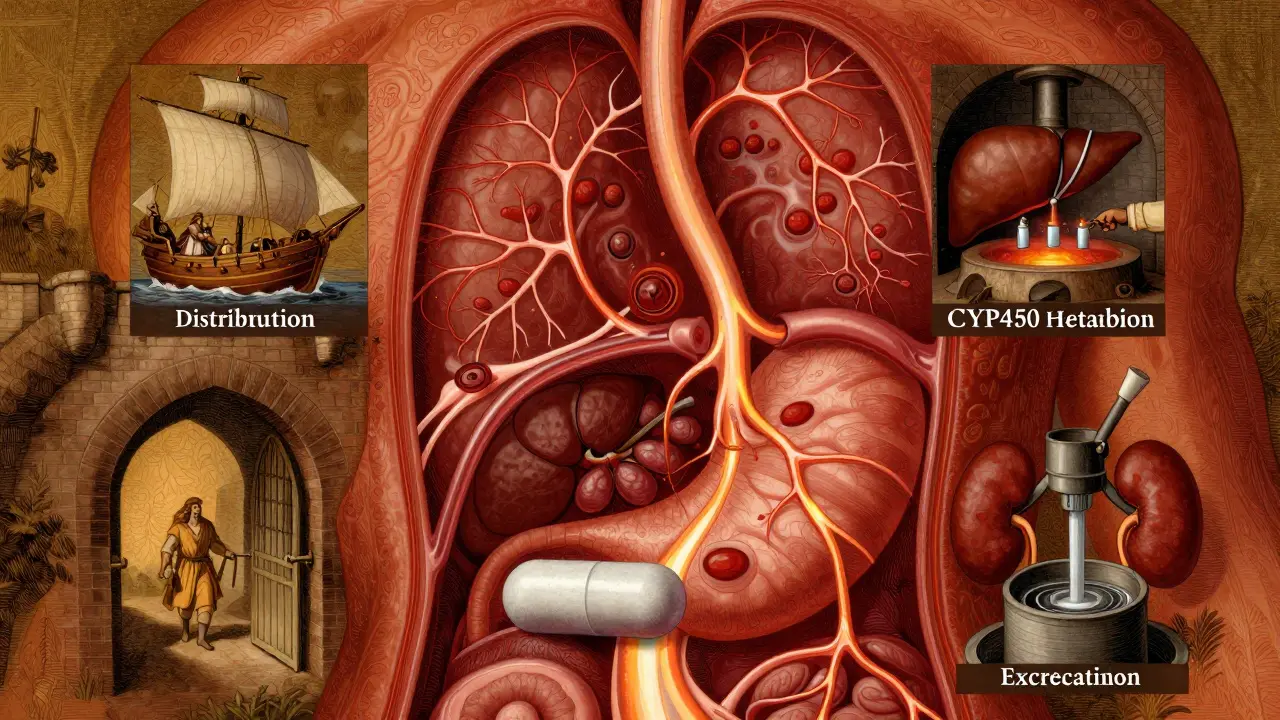
When you take a drug, whether it’s a pill, injection, or patch, your body doesn’t just accept it. It goes through four stages: Absorption, Distribution, Metabolism, and Excretion. Together, they’re called ADME. Think of it like a delivery system with checkpoints.
First, absorption. This is how the drug gets into your bloodstream. If you swallow a pill, it has to pass through your stomach and intestines. But not everything makes it. Your gut pH, how fast food moves through you, and even certain proteins like P-glycoprotein can block or slow absorption. For example, some antibiotics are absorbed 30-70% less if taken with calcium-rich foods. That’s why your doctor tells you to take certain meds on an empty stomach.
Not all drugs are swallowed. An IV shot? That’s 100% absorption - straight into your blood. A patch? Slow and steady. A nasal spray? Faster than a pill. The route changes everything.
Where Does the Drug Go?
Once in your blood, the drug gets distributed. This isn’t random. Some drugs stick to proteins in your plasma. Warfarin, for example, is 98% bound to albumin. That means only 2% is free to work. If another drug kicks off that bound warfarin, suddenly you’ve got too much active drug in your system. That’s how bleeding risks spike.
Other drugs slip into tissues - fat, muscle, even your brain. That’s measured by volume of distribution (Vd). A low Vd means the drug stays mostly in your blood. A high Vd? It’s soaking into your organs. That’s why some drugs affect your liver more than your heart, and why others make you drowsy even if they’re supposed to treat your joints.
Your Liver: The Drug’s Worst Enemy
Metabolism happens mostly in your liver. Enzymes - especially the CYP450 family - break down drugs so your kidneys can flush them out. CYP3A4 alone handles about half of all prescription meds. But here’s the catch: your genes decide how fast this enzyme works.
Some people are slow metabolizers. For example, 3-10% of Caucasians have a CYP2D6 variant that can’t turn codeine into morphine. They get no pain relief. Others are ultra-rapid - they turn codeine into morphine too fast. That’s how some people overdose on standard doses.
Drugs can also interfere with each other. Take clarithromycin (an antibiotic) with simvastatin (a cholesterol drug). Clarithromycin blocks CYP3A4. Simvastatin builds up. Risk of muscle damage? Goes from 0.04% to 0.5%. That’s a 12-fold increase. And most people don’t know they’re taking this combo.
How Your Body Gets Rid of It
Excretion is mostly through the kidneys. Your kidneys filter blood. If your kidney function drops - say, from age, diabetes, or dehydration - drugs don’t clear as fast. That’s why older adults get side effects more often. Their kidneys clear drugs 30-40% slower than younger people.
Normal kidney filter rate? 90-120 mL/min. In end-stage kidney disease? It can drop below 15 mL/min. That’s why vancomycin (an antibiotic) can cause kidney damage if dosed like it’s for a 30-year-old. A 78-year-old with a creatinine clearance of 25 mL/min? They need a much lower dose. But many hospitals still use standard charts. That’s how patients end up with rising creatinine levels and hospital stays.
Side Effects Aren’t Random - They’re Predictable
Side effects happen when drug levels go too high. Too low? No effect. Too high? Toxicity.
Phenytoin (an epilepsy drug) has a narrow window. At 10-20 mcg/mL? Works. Above 20 mcg/mL? 30% of patients get tremors, dizziness, even coma. At therapeutic levels? Only 2% have side effects. That’s why doctors check blood levels.
And it’s not always the original drug. Diazepam (Valium) breaks down into desmethyldiazepam - a metabolite with a 100-hour half-life. In young people? Fine. In elderly? It builds up. That’s why older adults fall more often on benzodiazepines. It’s not the drug. It’s the leftover stuff.
Warfarin? Another classic. A single gene variant in CYP2C9 can make you 5 times more likely to bleed on a standard dose. That’s why some clinics now test for it before prescribing. It’s not optional anymore - it’s standard practice for high-risk drugs.
Why Age, Weight, and Other Drugs Matter So Much
Here’s the truth: there’s no such thing as a standard dose. There’s only a starting point.
People over 65 have 30-50% less liver function. Their kidneys work slower. They’re often on 5+ meds. That’s why 1 in 3 adverse drug reactions happen in older adults. And it’s not because they’re “noncompliant.” It’s because the dose was never adjusted.
Obesity? Fat changes how drugs distribute. A 120kg person doesn’t need 2x the dose of a 60kg person - but they often get it. That’s because dosing is based on weight, but not on body composition. Muscle vs. fat changes drug behavior.
And what you eat? Grapefruit juice? It blocks CYP3A4. Same as clarithromycin. One glass can turn a safe statin dose into a dangerous one. It’s not a myth. It’s science.
What’s Changing Now? Personalized Dosing
Pharmacokinetics is no longer guesswork. It’s data-driven.
AI tools like DoseMeRx are now FDA-approved. They take your age, weight, kidney function, genetics, and current meds - then spit out a custom dose. For vancomycin, they cut dosing errors by 62%. That’s huge.
Regulators are catching up. The FDA now requires PBPK modeling (computer simulations of how drugs behave in virtual populations) for nearly all new cancer drugs. The EMA launched PK4All to build global databases for rare diseases. And the NIH is spending $185 million to fix the biggest gap: most pharmacokinetic studies still use young, white, male volunteers - even though 85% of patients aren’t.
Even your gut bacteria matter now. Researchers found 15-20% of oral drugs are changed by gut microbes before they even reach your liver. That’s why two people on the same drug can have totally different outcomes - one has a healthy microbiome, the other doesn’t.
What You Can Do
You don’t need to be a scientist to use this info.
- Know your meds. If you’re on warfarin, ask if your dose was adjusted for your age or kidney function.
- Tell your doctor about all supplements. St. John’s Wort? It speeds up metabolism. It can make birth control, antidepressants, or transplant drugs fail.
- Don’t ignore side effects. If you feel dizzy after a new drug, don’t just wait it out. Ask: “Could this be a pharmacokinetic issue?”
- Ask about testing. For drugs like clopidogrel, abacavir, or codeine, genetic testing is available and prevents serious reactions.
Medication isn’t one-size-fits-all. Your body isn’t a textbook. It’s unique. Understanding how it handles drugs isn’t just academic - it’s life-saving.
What does pharmacokinetics mean?
Pharmacokinetics is the study of how your body absorbs, distributes, metabolizes, and excretes a drug. It answers questions like: How much of the drug reaches your bloodstream? How long does it last? Where does it go? And how fast is it removed? This is different from pharmacodynamics, which looks at how the drug affects your body.
Why do some people have worse side effects than others?
Because everyone’s body processes drugs differently. Genetics affect how fast your liver breaks down meds. Kidney function changes with age. Other drugs can block or speed up metabolism. Even your diet and gut bacteria play a role. A dose that’s safe for one person can be toxic for another.
Can I test my body’s ability to process drugs?
Yes, in some cases. Genetic tests can identify variants in enzymes like CYP2D6 or CYP2C9 that affect how you metabolize common drugs like codeine, warfarin, or clopidogrel. Therapeutic drug monitoring (TDM) measures actual drug levels in your blood - often used for epilepsy meds, antibiotics, and antidepressants. These aren’t routine for everyone, but they’re standard for high-risk medications.
Does taking meds with food really matter?
Yes. Food can block absorption (like calcium with antibiotics) or boost it (like fatty meals with some HIV meds). Grapefruit juice blocks liver enzymes and can raise drug levels dangerously. Always check the label or ask your pharmacist. The timing and type of food can change how well your drug works - or how dangerous it becomes.
Why are older adults more at risk for drug side effects?
As we age, liver metabolism drops by 30-50%, and kidney clearance falls by 30-40%. Fat increases and muscle decreases, changing how drugs are distributed. Older adults also take more medications - increasing the chance of dangerous interactions. What was a safe dose at 40 might be toxic at 75. Doses should be lowered, not just repeated.
Is pharmacokinetics only for serious drugs?
No. Even common drugs like ibuprofen, acetaminophen, or antihistamines can build up if your kidneys are slow. A 70-year-old on daily ibuprofen for arthritis might not realize their kidney function has dropped. That’s how liver damage or stomach bleeding happens. Pharmacokinetics matters for every medication - not just the ones on black-box warnings.
Final Thought
Your body isn’t a machine with a fixed setting. It’s a living system. And drugs? They’re chemicals that interact with it - sometimes beautifully, sometimes dangerously. The better you understand how your body handles them, the safer you are. Ask questions. Demand better. Your life depends on it.
Shalini Gautam
February 22, 2026 AT 04:45So glad someone finally broke this down without jargon. In India, we see so many people taking antibiotics with milk or yogurt-no idea it kills absorption. My aunt took doxycycline with her morning lassi and wondered why her infection never cleared. Simple fix: wait 2 hours. But no one tells you this.
Pharmacokinetics isn’t just science-it’s survival. And yeah, our grandparents are dying because dosing charts were made for 25-year-old white guys in 1987. Time to update the system.
Erin Pinheiro
February 23, 2026 AT 15:15ok so like… i just read this and im like wow i never knew my body was this complicated?? like i take tylenol every day for my back pain and now im scared to even breathe??
also why does grapefruit juice have to be such a drama queen?? it’s not even a drug but it ruins everything??
Brandice Valentino
February 25, 2026 AT 13:02Let’s be real-most of this is common sense if you’ve taken a single biochem class. But I guess the average person thinks their body is a magic box that just ‘absorbs’ pills like a sponge. Cute.
Also, the fact that we’re still using ‘standard doses’ in 2024 is a crime. My cousin got hospitalized because her doctor didn’t adjust her warfarin for her 72-year-old kidneys. She’s fine now. But she shouldn’t have had to fight for basic care.
And yes, gut microbiome matters. I’ve seen people on identical regimens have wildly different reactions because one had a Crohn’s flare and the other ate kimchi daily. Science is wild.
Larry Zerpa
February 26, 2026 AT 17:49There’s a fundamental flaw in this entire narrative: pharmacokinetics is not the primary driver of adverse drug reactions. It’s the regulatory capture of pharmaceutical companies and the systemic abandonment of clinical pharmacology in medical education.
Doctors don’t prescribe poorly because they’re ignorant of ADME-they prescribe poorly because they’re incentivized to prescribe more. The FDA approves drugs based on industry-funded trials with homogeneous populations. The NIH spends $185 million? That’s pocket change compared to the $12 billion the industry spends annually lobbying for one-size-fits-all dosing.
Personalized dosing isn’t the solution-it’s a distraction. The solution is dismantling profit-driven medicine. Until then, your ‘data-driven’ AI tools are just algorithmic band-aids on a hemorrhaging system.
Gwen Vincent
February 28, 2026 AT 00:59This is so important. I’m a nurse and I see this every shift. A 78-year-old woman on 8 meds, including a statin and an antibiotic, and no one checked for interactions. She ended up with rhabdomyolysis. It’s not her fault. It’s not the doctor’s fault. It’s the system.
Thank you for writing this. I’m sharing it with my team. Maybe if we all start asking the right questions-‘Did we consider her kidney function?’ ‘Is this dose appropriate for her weight?’-we can start changing things.
Also, yes, grapefruit juice. Always ask. Always.
Nandini Wagh
March 1, 2026 AT 18:26Wow. So basically, if you’re not a rich white man in your 20s, your body is just… broken? Like, I take melatonin every night and now I’m terrified I’m slowly poisoning myself because my gut bacteria are ‘bad.’
Also, why does this article sound like a pharmaceutical ad? ‘Ask your doctor about genetic testing!’ Yeah, because that’s totally affordable for the 70% of people who can’t afford their insulin.
Holley T
March 2, 2026 AT 03:29Okay, I’ve been reading this article for 20 minutes and I need to say something. The idea that ‘there’s no such thing as a standard dose’ is both true and terrifying. But let’s not pretend this is new. I’ve been telling people since 2018 that dosing is a joke. I’m a biochemist. I’ve worked in clinical trials. We know this.
What’s not being said? The cost barrier. Genetic testing for CYP2D6? $400. Therapeutic drug monitoring? $200 per test. Insurance won’t cover it unless you’re on a ‘high-risk’ drug. Which means if you’re on ibuprofen for arthritis? Too bad. You’re just supposed to suffer quietly until you get a GI bleed or kidney failure.
And don’t get me started on how little is done for non-white populations. Most PK studies still use 18-35-year-old males. We’re not even trying. We’re just pretending we are.
Also, the gut microbiome thing? It’s not 15-20%. It’s closer to 30% for certain drugs. The data’s out there. No one’s acting on it. Because money.
Ashley Johnson
March 3, 2026 AT 08:30I don’t trust any of this. I’ve read that the FDA is controlled by Big Pharma. They’re pushing this ‘personalized dosing’ nonsense to sell more tests and more drugs. What if your genes are fine but your body is just… poisoned by 5G? Or glyphosate? Or the vaccines? I’ve seen people get sick after taking one pill and they never had issues before. Coincidence? I think not.
Also, why do they always say ‘your doctor’? Who’s your doctor? The one who gets paid per prescription? I think they’re lying to us. The real reason some people have side effects is because their bodies are rejecting toxins from the food supply. Not pharmacokinetics. It’s all about toxins. And they don’t want you to know that.
tia novialiswati
March 5, 2026 AT 07:38OMG YES THANK YOU FOR THIS!! 🙌 I’ve been on antidepressants for 8 years and my doctor finally switched me after I told him I felt like a zombie. We did a TDM test and my level was 3x higher than it should’ve been. I had no idea!!
Also, I started taking St. John’s Wort for anxiety and didn’t tell my doctor. Turns out it made my birth control useless. 😳 So embarrassing but so important.
Ask questions. Tell your doctor everything. Even the weird stuff. You’re not weird-you’re smart. 💖
Valerie Letourneau
March 5, 2026 AT 18:08While the scientific foundation presented here is commendable, I must underscore the profound ethical imperative to ensure equitable access to pharmacokinetic diagnostics. In Canada, we have publicly funded therapeutic drug monitoring for select agents, yet disparities persist in rural and Indigenous communities.
The integration of AI tools such as DoseMeRx is promising, but without mandatory inclusion of diverse phenotypes in training datasets, we risk amplifying existing health inequities. The NIH’s $185 million initiative is a step forward-but it must be paired with structural reforms in medical education and regulatory policy.
Pharmacokinetics is not merely a biological phenomenon; it is a social determinant of health.
Khaya Street
March 7, 2026 AT 12:57This is solid. As a healthcare worker in South Africa, I see this daily. A 65-year-old man on ten meds, including simvastatin and clarithromycin-no one checked his creatinine. He ended up in ICU with rhabdomyolysis. We don’t have AI tools. We don’t have genetic testing. We just have a chart and a prayer.
But here’s the thing: even with limited resources, asking three questions changes outcomes-‘What else are you taking?’ ‘Are you eating grapefruit?’ ‘Have your kidneys been checked?’
Knowledge isn’t just power. It’s the difference between life and death.